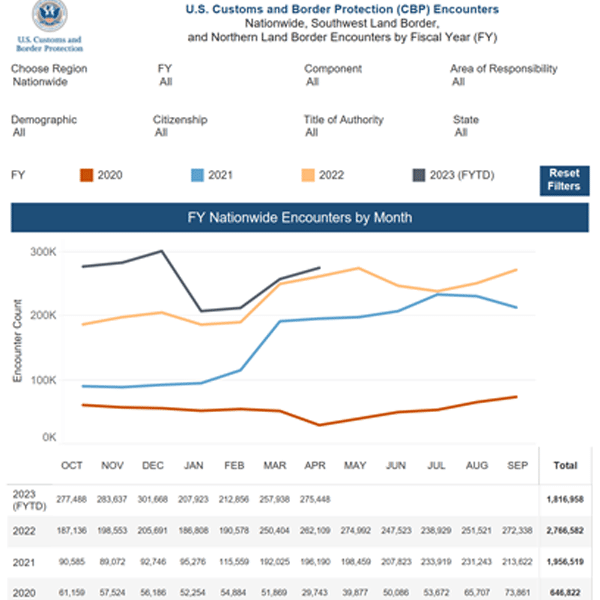
CBP Nationwide Encounters by Month (2020 to April 2023)
The data clearly illustrates when the invasion started. Yes, there will always be those who attempt entry, but this administration played a direct role in
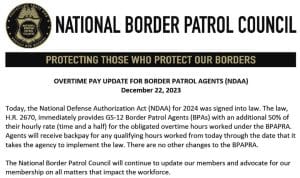
Overtime Pay Update for Border Patrol Agents (NDAA)
Today, the National Defense Authorization Act (NDAA) for 2024 was signed into law. The law, H.R. 2670, immediately provides GS-12 Border Patrol agents (BPAs) with



